December 2025 – This new chapter contains guidance on when a Large-Scale Enquiry (LSE) should be held, and outlines the processes involved from decision to initiate an LSE through to quality assurance and learning.
CONTENTS
Executive Summary
Safeguarding means protecting an adult’s right to live in safety, free from abuse and neglect, as well as promoting good practice for responding to concerns on a multi-agency basis. The Care Act 2014 sets out the Local Authority and partner organisations’ responsibilities for protecting adults with care and support needs from abuse or neglect. All Large-Scale Enquiries (LSE) are carried out under the statutory framework of Section 42 of the Care Act 2014. This involves working in partnership with individuals and organisations.
The implementation of the Local Safeguarding Adults Board Protocol for managing an LSE, is a collaborative responsibility for which all agencies are accountable. The procedure applies to all care and support provisions, other than prisons and approved premises, whether directly commissioned or not by a Local Authority or Integrated Care Board (ICB)/Integrated Care Partnership (ICP) or NHS England, and irrespective of whether it is included in the Care Quality Commission (CQC) market oversight. Services managed by the Local Authority or NHS are subject to the same level of scrutiny as independent care providers.
This protocol complements and supplements the Buckinghamshire Safeguarding Adults Board (BSAB) Multi-Agency Safeguarding Policy and Procedures. It seeks to outline what determines an LSE and provides guidance on the response that is required in such situations.
An LSE could be triggered where there are significant concerns and/or a high level of safeguarding activity in relation to adults at risk or where there is a complex concern regarding a number of adults at risk that requires a multi-agency response, e.g. one or more person(s) alleged to have caused harm in relation to multiple victims who are adults at risk.
This procedure should be reviewed and amended in the light of experience and lessons learned from undertaking LSE as appropriate.
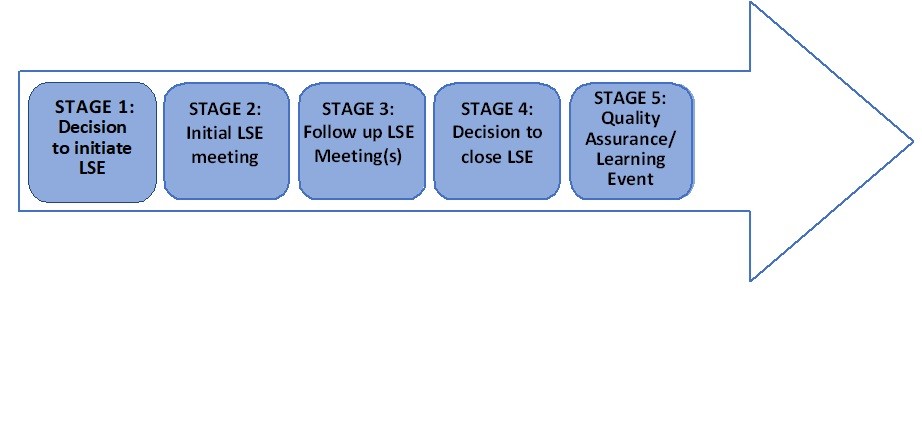
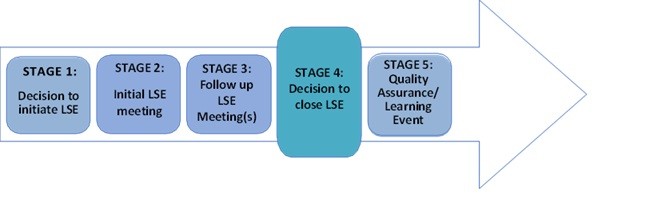
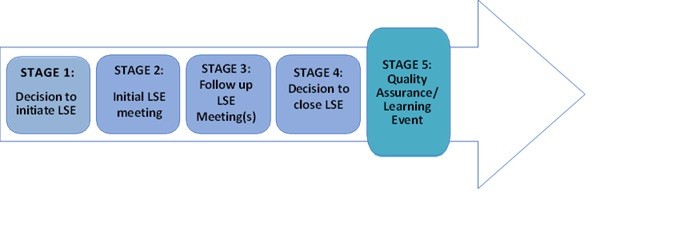
The five stages of an LSE will be detailed throughout the protocol as follows (click on the image to enlarge it):
1. Guiding Principles
Whilst Buckinghamshire Council Adult Social Care have a duty to co-ordinate safeguarding enquiries, effective responses to large-scale concerns must be based on multi-agency responses. This results in collective responsibility and shared accountability across agencies.
Individual safeguarding concerns need to be addressed via individual safeguarding processes; it is not a replacement for the management of individual concerns and will run parallel to the LSE.
All agencies receiving safeguarding concerns need to consider the possibility of more than one adult who may potentially be at risk. It is essential that collaborative working and appropriate sharing of information across agencies takes place to identify information about any previous enquiries and allegations involving any named individuals or the organisation.
As with any safeguarding enquiry, the governing principles of safeguarding apply and must be followed as the concerns are investigated. These are:
- that the voice of the adult is heard, and their lived experience understood and what they have to say is taken seriously and acted upon in an appropriate manner;
- individuals have a right to privacy; to be treated with dignity and to be enabled to live an independent life;
- everyone’s circumstances are different. Individuals should be able to exercise choice about how they lead their lives and have their rights upheld, regardless of ethnic origin, gender, sexuality, disability, age, religious or cultural background and beliefs;
- intervention should be proportionate to the harm or possibility of future harm, and which has the overall effect (outcome) of improving the life of the adult(s) at risk and balanced with public interest;
- all responses to safeguarding concerns should consider an outcome which supports or offers the opportunity to develop or to maintain, a private life which includes those people with whom the adult wishes to establish, develop, or continue a relationship and a right to make an informed choice.
Where adults lack capacity to safeguard themselves, other people will need to make those decisions. In such cases, there will need to be a consideration for advocacy support. In doing so, they will act as decision maker and will make “best interest decisions” on their behalf in accordance with the Mental Capacity Act 2005 and associated Code of Practice.
Where it is suspected that a crime may have been committed the police must be alerted at the earliest possible opportunity.
2. Organisational Abuse and Neglect
The Care and Support Statutory Guidance highlights the seriousness of organisational abuse, which can include neglect and poor care practices within various care settings. This type of abuse violates a person’s dignity and human rights. Abuse and neglect can range from isolated incidents to pervasive ill treatment, whether intentional or unintentional. Concerns about organisational abuse may arise from various sources, such as accumulated complaints, serious safeguarding concerns, reports from professionals, and failure to engage in safeguarding activities. If there is clear evidence of ongoing harm despite monitoring and action planning, further action may be necessary to protect adults at risk.
All Organisations must follow their own system wide escalation framework and monitoring processes prior to initialising an LSE.
3. Potential Triggers for a Large-Scale Enquiry
If there is a concern that the criteria may be met, a pre-meeting should be held. A list of examples of when the criteria are met include:
- one incident or concern occurs that indicates that systemic safeguarding concerns may exist that affect multiple adults using the service;
- where there is a public or vital interest;
- a series of safeguarding and/or quality concerns have been raised about the same organisation and/or unit that indicate systemic concerns This could include care provided in people’s own homes. These may include concerns in relation to the overall standards of care, for example omissions in care, safeguarding concerns/enquiries, a lack of risk management processes, a lack of leadership issues, and staffing concerns, as well as a lack of governance procedures, including missed calls, ineffective recording and reporting’
- where a provider is found to require improvement or inadequate following a CQC inspection;
- a one off concern of such severity, for example a choking incident that caused a death, fall with harm, lack of pressure ulcer Where it is considered that this failure would be judged to present significant risks to others receiving care by the same provider;
- poor quality care following a quality assurance audit and lack of response from the provider to recommendations/actions.
- Failure to comply with contractual obligations.
This is not an exhaustive list. Professional judgement should always be used to determine the most proportionate response.
An LSE triggers, analysis and evidence document is available in Appendix 1.
During the course of an LSE, individual adult safeguarding Section 42 enquiries will continue alongside to ensure individual adults identified as at risk are safeguarded.
4. LSE Flowchart
Large-scale Enquiry Process – Flowchart (opens as a PDF)
5. The Role of the Large-Scale Enquiry Chair
The Chair of the LSE will be the Local Authority Operational Lead or nominated senior manager in Adult Social Care. The key responsibilities of the Chair are to:
- arrange LSE meetings as required (the frequency of the subsequent meeting to be agreed at the end of each meeting);
- secure appropriate membership and representation at all LSE meetings;
- consider the appropriateness and timing of care provider involvement;
- ensure the highest level of confidentiality and appropriate information sharing;
- ensure that there are explicit records of decision-making;
- promote best practice levels of multi-agency working;
- ensure relevant stakeholders are updated and there is an opportunity for staff to have regular check-ins to ensure their well being and to gather information relevant to the enquiry;
- ensure that the views and wishes of the adults at risk and their families/representatives are considered throughout;
- ensure an overview of actions (including those established at the pre-meet) and outcomes and ensure actions are progressed in a timely manner;
- notify the CQC inspector, if the service is registered;
- communicate with the provider and ensure they are aware of the requirement to produce an action plan;
- ensure police led enquiries are included to ensure best evidence and manage pending investigations;
- ensure that there is an overarching action plan and risk assessment.
6. Engagement with Adults at Risk, their Relatives and / or Representatives
When a decision is taken to proceed to LSE, the adult(s), and their family/representatives (with consent), should be formally contacted via letter or email to advise that safeguarding concerns have been raised and enquiries are being This will be undertaken by the provider and the content of the letter/email agreed with the LSE Chair before it is sent. Care must be taken at this stage to ensure that any direct contact is based on factual information reflecting the Duty of Candour (Section 81 Care Act 2014) (Regulation 20 Health and Social Care Act 2008 (Regulated Activities) Regulations 2014).
If an adult at risk is funded by another local authority, agreement should be sought as to who will contact family/representatives with the funding authority.
Initial contact must be made as soon as possible after the decision to proceed with an LSE has been made and include agreed points of contact for further information. This will usually include details for the provider and the Chair of the LSE. Records of contacts must be made by the provider adhering to data protection policy and procedures. Copies of any written correspondence are shared with the LSE Chair.
For adult(s) at risk who have mental capacity, their consent should be sought and recorded regarding what information can be shared with relatives/representatives, or Care Act Advocate.
If the adult(s) at risk lacks mental capacity to consent to the sharing of information and has no Lasting Power of Attorney or Deputyship for Personal Welfare, then a best interests decision should be reached regarding who is the most appropriate representative to be contacted. This could be for example a family member, friend or IMCA service.
7. Referrer
Consideration should be given to how the person making any initial referral is involved in the This will vary depending on the circumstances of the case. However, in all cases the Core Group will determine a mechanism and frequency of feedback to the referrer, having regard for confidentiality, about the progress of the LSE.
All agencies involved should refer to their own Whistleblowing Policy and Procedures. Where a concern is raised by a whistleblower, the person receiving the concerns should ensure that the whistleblower has followed their own organisation’s whistleblowing procedures. Information should be obtained from the whistleblower as to whether they want their anonymity maintained.
Although all efforts should be made to ensure this, they must be advised that this cannot always be guaranteed. Where a whistleblower does not wish to leave their contact details it is vital wherever possible that as much detailed information is obtained in relation to any specific service users or incidents to support an investigation to take place.
Further information for whistleblowers can be obtained from the following websites:
- Public Concern at Work – an independent Whistleblowing Charity.
- Speak Up – free, independent, confidential advice on the speaking up process
- Whistleblowing for Employees (gov.uk)
- Raising a Concern with CQC: A Quick Guide for Health and Social Care Staff about Whistleblowing
8. The Role of the Provider of Concern
In most cases of LSE it is important for the provider to be involved in undertaking certain elements of the enquiry.
Clear information must be given to the provider regarding the nature, reasons for, and timescales of LSE and individual section 42 enquiries along with realistic outcomes, including their responsibilities.
Partnership working with the provider is crucial. This includes (but is not limited to) working with the provider in ensuring information is provided regarding individual adults at risk in respect of their names, the authority funding their placement or if they are self-funding, the adult’s representative and/or their next of kin.
Any support/assistance necessary in undertaking any individual enquiries.
Assist in the LSE through the provision of written reports, any findings and recommended actions.
To provide, if requested, a detailed action plan, including milestones and review dates, setting out how service deficiencies will be mitigated. Any action plan should capture the requirements of the council, ICB and Care Quality Commission to avoid duplication and multiple plans.
Provide appropriate representation at Large Scale Enquiry meetings.
Ensure adherence to any agreement made during the LSE process including those relating to embargoes and responsibilities for ensuring that the individual, and other stakeholders are kept informed of any organisational safeguarding proceedings taking place.
Where there are concerns of provider failure, this should include details of the support that the provider is delivering. If the LSE identifies that there is a risk of provider failure this information must be shared with the Lead Commissioner immediately. The Local Authority will implement their provider failure policy to ensure that there is effective management of this identified risk.
Any emergency action, including consideration for ceasing commissioning arrangements, may be taken by the local authority in line with their commissioning and contract monitoring framework.
While appropriate and co-operative behaviour by the provider is expected, it may not always be appropriate to delegate an enquiry to the provider. This will be discussed at the LSE initial meeting. However, due regard will be given to the provider’s own mechanisms, such as disciplinary procedures, and how any intention to deploy these relates to the safeguarding concerns and aligns to any pre-existing action plans
Provider’s also need to clarify any intended use of legal representation of providers.
9. Purpose of the Initial LSE Meeting
9.1 Planning and operational decisions
- determine whether to progress with the LSE;
- act to ensure the safety of all adults at risk – this may include taking action to suspend or relocate staff;
- consider the need for alternative accommodation or care provision for any adults who may require this. Cross-referencing the provider failure policy if relevant;
- whether any criminal offences are identified and whether any criminal investigations are being progressed. Any Police investigation will take primacy. However, other enquiries (of a health or social care nature) may run along in parallel where appropriate. It should be agreed by all partner agencies, the level and scope of all strands of the LSE;
- whether there are any open coroner cases;
- co-ordinate the Enquiry Action Plan and who has overall responsibility for co-ordination;
- to avoid drifts, there will need to be clear timescales and agreement as to the format and presentation of information;
- the Provider must create an action plan to address all areas of concern;
- using the SBAR template (Appendix 9) may be useful as it is a structured communication method that stands for Situation, Background, Assessment, and Recommendation. it is now used to transfer critical information clearly and concisely, especially in urgent situations, to improve patient safety and facilitate efficient patient handovers;
- set out the roles and responsibilities of each organisation and individuals involved, ensuring that all are aware of how their contribution to the enquiry fits into the overall multi-agency process and any other concurrent processes;
- challenge partners where necessary. Where they are or appear to be unwilling to actively participate in the enquiry, escalate the concern within a partner’s own organisation as detailed in the Multi-Agency Safeguarding Adults Policy and Procedures;
- consider the support needed by staff throughout the enquiry process;
- ensure that actions and outcomes are fed into any individual section 42 enquiry plans for adults at risk;
- set timescales and framework for ensuring all actions are completed;
- consider whether the criteria for Safeguarding Adults Review referral has been met;
- what steps are to be taken to assure the adult’s safety in future;
- the provision of any support, treatment or therapy including on-going advocacy;
- how best to support the adult through any action they take to seek justice or redress.
9.2 Good practice / principles
- due regard needs to be given as to whether the individuals can give valid and informed consent as part of the LSE process, or if there is reason to doubt their ability to make such a decision, whether the principles of the Mental Capacity Act need to be applied;
- information sharing and information governance requirements (referring to each organisation’s policy and procedures);
- the need to involve independent advocacy as determined under the Care Act 2014 Care and Care and Support Statutory Guidance, an Independent Mental Capacity Advocate (IMCA) see the Mental Capacity Act Code of Practice (chapter 10) or an Independent Mental Health Advocate if they are subject to the Mental Health Act 2007 (Chapter 4 of the Mental Health Act Code of Practice);
- how to support the adults at risk and their family/carers/representatives through the enquiry process, in line with the principles of Making Safeguarding Personal (see Making Safeguarding Personal chapter);
- proportionate intervention with the least intrusive response appropriate to the risks presented;
- ensure transparency and clear lines of accountability in the conduct of the enquiry.
9.3 Communication
- consider the need for an overall communications strategy, including potential media contact;
- share information with other organisations that may need to be involved or kept informed; for example, commissioners from different geographical areas;
- share information with the adults who receive a service, their families and their representatives;
- consider who needs to be notified of the enquiry within the Local authority, including legal services, elected members and communications departments;
- to act as a conduit of communications for all partner agencies at a local and national level;
- communication with the Nominated Individual for the Provider and Registered Manager.
9.4 Outcomes / planning
- how to request and receive reports and information;
- identify further areas for improvement and develop action plans as appropriate;
- monitoring of progress, and the safety and well-being of adults;
- whether the nature of the concerns meet the criteria for referral for a Safeguarding Adults Review (SAR);
- ensure that actions and outcomes are fed into the section 42 enquiry plans for individual adults at risk;
- determine the need for follow up meetings;
- planning and coordination of any police investigations.
10. Recording of Minutes and Storage of Documentation (Data Protection)
All LSE meetings will be minuted or digitally recorded. Minutes and actions will be circulated in draft format and agreed at subsequent meetings. All LSE meetings must have formal notes taken by administrative staff who have been trained in note taking.
Minutes and documentation must be kept securely by all parties.
Due to the sensitive nature of LSE, care must be taken by all participants to keep information that they receive as part of the investigation, safe, secure and confidential at all times and in accordance with their organisation’s policies and procedures. When sharing information by email, organisations must ensure that information is only sent through an encrypted email system, and anything sent by external post goes by recorded delivery.
All breaches of confidentiality must be reported with immediate effect to Buckinghamshire Council’s Data Protection Officer, Adult Social Care Service Director (Operations) and the LSE Chair. If there is doubt about the sharing / disclosure of information, please refer either to the LSE/Designated Chair or refer to your own organisation’s local information governance policies and procedures.
Information shared should only be for the legitimate purpose of safeguarding individuals and families.
Information shared at safeguarding meetings is for that purpose only and should relate only to the individual(s) / organisation / agency concerned.
The distribution of the notes from the meeting should be agreed at the meeting and will be confirmed with those present.
Notes will be sent out within 10 working days of the meeting and sent via either secure email or password protected. They will not be reproduced or distributed more widely without the express permission of the LSE Chair.
All information should be stored securely both electronically and or in paper form in line with organisational policies and the Data Protection Act 2018. For Buckinghamshire Council, organisational based information will be stored in a designated secure area and personal based information will be stored in Adult Social Care’s electronic client recording system.
11. Stages of the Large-Scale Enquiry
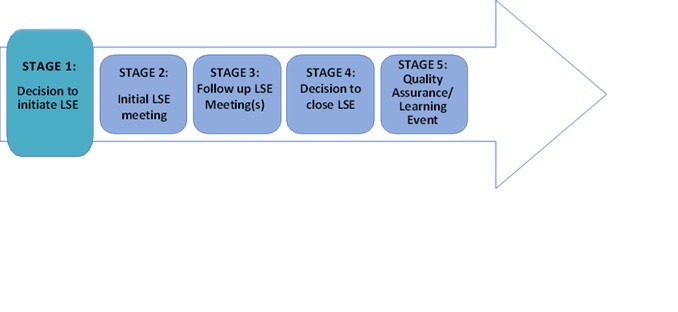
11.1 Stage 1- the concern, information sharing and decision making stage (to commence immediately)
There are a number of routes through which concerns indicating the need for an LSE might be identified and then refereed on, and these are specific to the following service areas:
-
- Adult Social Care Operational Teams;
- Adult Social Care Commissioning and Partnerships;
- Adult Social Care Safeguarding Team.
The authority for initiating an LSE rests with the Local Authority Operational Lead for Adult Safeguarding or in their absence a more senior officer.
Buckinghamshire Council is responsible for all LSEs within it’s county. For care homes this should be clear, however, it can be the case that Domiciliary/Home Care Providers will have their registered base in another Local Authority’s area (the host area), but predominantly provide their service in another Local Authority’s area. Therefore, where it is the case that the concerns are identified in a non-host Local Authority’s locality, there needs to be consultation between representatives of both local authorities to make a decision about which Local Authority leads the LSE. This decision needs to take into account evidence of the concerns known to each Local Authority.
If the concern relates to a service commissioned exclusively by an ICB/ICP then the decision to implement the LSE procedure should be made in conjunction with the Local Authority Operational Lead for Adult Safeguarding, the Continuing Health Care Representative, and/or the Designated Nurse for Adult Safeguarding from the ICB. It is for the local authority to determine the appropriateness of the outcome of an enquiry. Once enquiries are completed, the outcome should be notified to the local authority which should then determine with the adult what, if any, further action is necessary and acceptable’. This is also the case where the local authority causes the health provider to make an enquiry.
Once sufficient information is available, the Local Authority Operational Lead for Adult Safeguarding, or in their absence a more senior officer, will make a decision whether to progress to an LSE within 24 hours. The safety and well-being of adults at risk is paramount at all stages of the process and all practicable steps must be taken to avoid delay.
Early discussion, in the form of a pre-meet, with the Head of Safeguarding is advised.
The decision to initiate an LSE should be communicated to all relevant internal and external contacts and partner agencies.
Where there is dispute or disagreement regarding decisions made about or within an LSE, the BSAB Escalation and Resolution Protocol should be used to consider or inform potential action.
Once the decision has been made to initiate the LSE, the following actions should be taken promptly and overseen by the Local Authority Operational Lead for Adult Safeguarding, or in their absence a more senior officer:
-
- immediate actions to ensure adults are adequately safeguarded;
- information shared with those that need to know;
- appointment of an LSE Chair;
- arrange an initial planning meeting.
11.2 Stage 2- large scale enquiry meeting
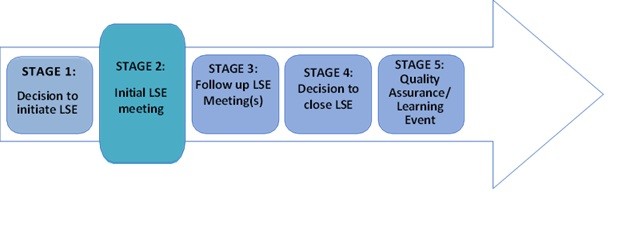
It is imperative that a meeting be held with all relevant agencies at the earliest opportunity and within five working days of the decision to progress to an LSE. The purpose of the initial meeting is to decide what action needs to be taken and by whom.
The core group for Large Scale Enquiry includes:
- Local Authority Adult Service Manager or a senior manager where the provider is based (lead local authority);
- representatives of other funding authorities where care is commissioned from the provider;
- Team Manager for Adult Social Care;
- Local Authority Adult Safeguarding specialist;
- relevant Safeguarding lead for local Health Trusts, and providers (including primary care and SCAS);
- Thames Valley Police (TVP);
- Care Quality Commission (CQC);
- senior Commissioning Manager from Health and Social Care;
- senior Provider representation e.g., Nominated Individual/ Registered Manager/ Directors etc.;
- other Local Authority/ Funding Commissioners;
NB: There may be occasions where meetings with the provider may be held outside the core group meetings. This decision will be made by the Chair.
On a case-by-case basis, as appropriate other representatives could include:
- representatives of other commissioners of services;
- legal representative from the Local Authority;
- Healthwatch;
- probation;
- advocacy services / IMCA service;
- representative from Children’s Services;
- health providers;
- Primary Care Network;
- Out of Hours GP;
The Chair is responsible for ensuring that partner and provider agencies have an appropriate level of seniority in attendance, and that their attendance at LSE meetings is consistent. Providers which have services on multiple sites should assign the area/regional manager; smaller providers the registered manager; voluntary sector the chairperson and manager/CEO of the trust or management committee.
This process is subject is subject to information sharing and data protection procedures. All parties must seek permission from the Chair to share any information relevant to the LSE outside of the core group identified.
11.3 Stage 3- review meeting (to be held within 28 days of commencement of enquiry and every 28 days until closure)
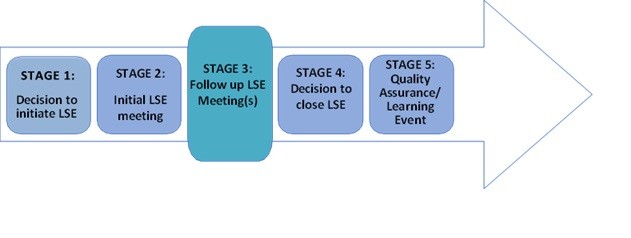
The purpose of the review LSE meeting is to share the findings of the various strands of the enquiries undertaken, reach broader conclusions about the nature and extent of the alleged abuse within the service and ensure an improvement plan is in place.
All those who attend the review LSE meeting are required to ensure that they have completed the actions agreed at the initial or previous LSE safeguarding meeting and have provided the Chair with a report prior to the meeting, or as a minimum requirement have the information available to share at the review LSE safeguarding meeting in a format that complies with Data Protection Act 2018 requirements.
The relevant provider manager should be invited to attend the review LSE meeting as it is vitally important that they are fully engaged with undertaking an active role with the improvement plan.
Review meetings will adhere to the same process and principles as initial meetings.
11.4 Large-scale enquiry closure
LSE safeguarding procedures will be closed when there is sufficient evidence demonstrating concerns have been addressed and sustained care quality improvements have been made. Any disputes over the decision to close should follow the BSAB Escalation and Resolution Protocol.
When the enquiry is closed the following steps need to take place:
- a letter sent to all affected adult(s), family members and agencies from the Chair informing them of the outcomes and closure of the enquiry and the process for raising any further enquiries;
- letter to other commissioning authorities informing them of the closure;
- consider what ongoing quality monitoring is required;
- letter to the service provider informing them the enquiry has been closed, the outcomes, and plans for reinstatement of business (where commissioning has been suspended). This needs to align with contract action;
- feedback to the referrer where appropriate;
- feedback to relevant organisations e.g. CQC, ICB, NHS England, Monitor, Healthwatch;
- Where serious concerns or themes requiring multi-agency strategic oversight have been identified, a summary report should be sent to the Buckinghamshire Safeguarding Adults Board by the Chair. The report can include themes of incidents, agencies involved, outline of concerns and summary outcomes of enquiries.
Each agency will have its own internal governance structure to monitor the actions identified through the LSE safeguarding process and will be accountable for actions assigned to individual agencies. For example, providers have the responsibility to refer employees to the Disclosure and Barring Service (DBS) and professional bodies. This should be considered at the conclusion of any disciplinary matters. The Disclosure and Barring Service exists to prevent unsuitable people from working with adults at risk and children.
NB – the local authority retains responsibility and accountability where it has ‘caused enquiries’ to be made until all necessary action has been taken to resolve the risks. The decision to end an LSE should be made by the Local Authority Operational Lead in consultation with core partners.
11.5 Quality assurance / sustainability of change
Throughout the whole of the LSE process, the aim is to embed sustainable change to improve the quality of the service provision. Quality assurance following closure of the LSE will be required from the provider organisation to demonstrate this, alongside monitoring from the Local Authority and Commissioners. Each Local Authority and partners will have their own mechanisms for this.
Any learning identified is to be shared as required with partner agencies. Learning could include quality of care issues as well as learning about the LSE process. Feedback should be sought from all partners as well as the adults and their families/carers or advocates.
A learning event may be convened by the BSAB where appropriate.
Due to the complexity often with the LSE process it should be a consideration that a regular forum for stakeholders is arranged. This provides an opportunity for stakeholders to decompress and reflect on the process.
12. Relevant Guidance
Care and Support Statutory Guidance
13. Appendices
Appendix 1 – Large scale enquiry triggers, analysis and evidence document
Large Scale Enquiry Triggers, Analysis and Evidence Document (opens in Word)
Appendix 2 – Initial LSE Planning Meeting Template
LSE Initial Planning Meeting Agenda (opens in Word)
Appendix 3 – LSE Enquiry Report Template
LSE Enquiry Report Template (opens in Word)
Appendix 4 – LSE Review Meeting Agenda
LSE Review Meeting Agenda (opens in Word)
Appendix 5 – LSE Letter Templates
LSE Letter Templates (opens in Word)
Appendix 6 – Organisational Safeguarding Plan Example
Organisational Safeguarding Plan Example (opens in Word)
Appendix 7 – LSE Provider Meeting Notes Template
LSE Provider Meeting Notes Template (opens in Word)
Appendix 8 – Large Scale Enquiry – Professional Partnership Meeting notes template
Large Scale Enquiry – Professional Partnership Meeting notes template (opens in Word)
Appendix 9 – SBAR Template
SBAR (strengths, background, assessment and recommendations) Report Template (opens in Word)